North Dakota Ems Patient Care Report Template
North Dakota Ems Patient Care Report Template
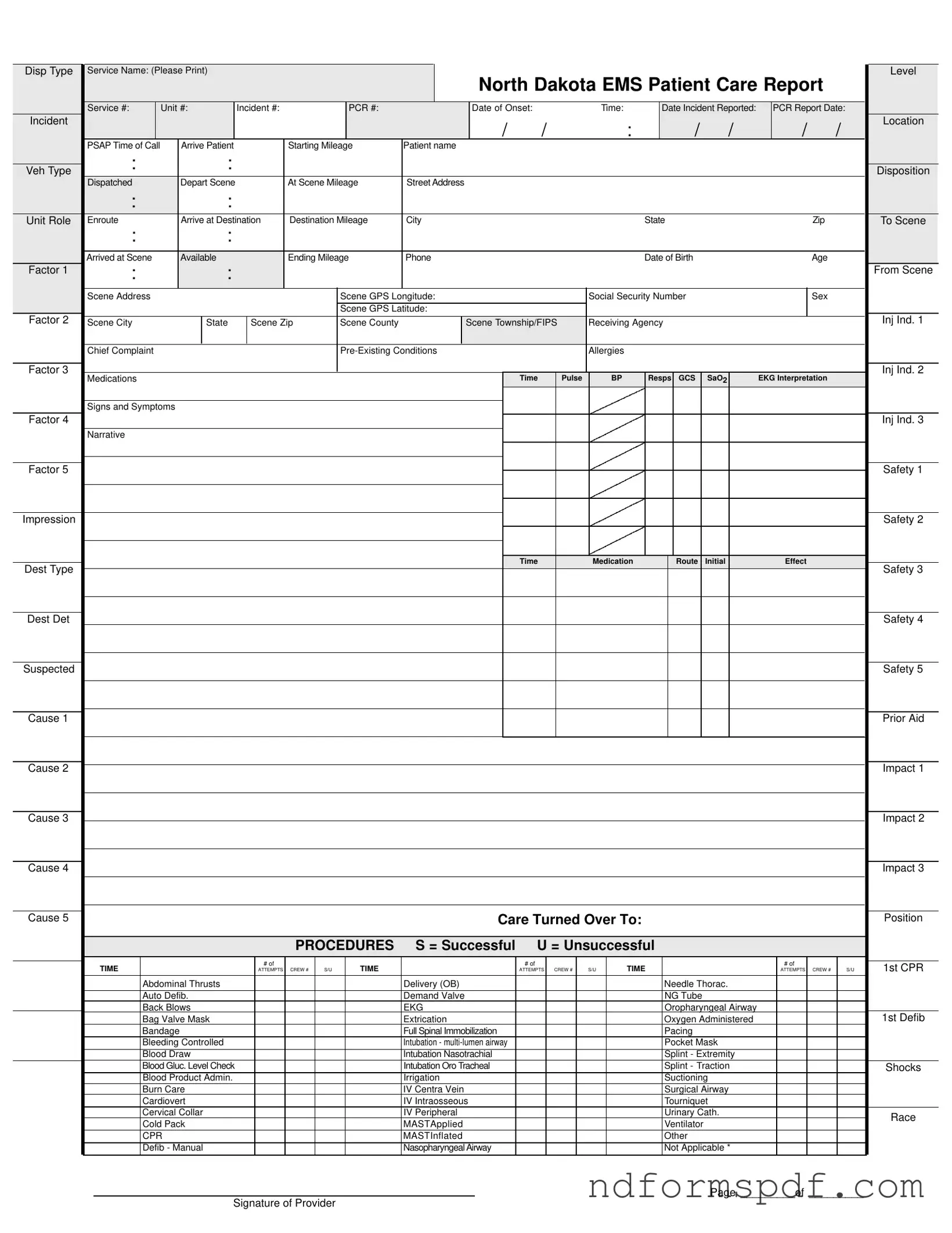
The North Dakota EMS Patient Care Report form is a vital document that captures essential information during emergency medical services. This form includes fields for identifying the service name, unit numbers, and incident details, ensuring that all relevant data is recorded efficiently. It asks for the patient’s name, date of birth, age, and social security number, which are crucial for patient identification and care. The form also captures the chief complaint, pre-existing conditions, allergies, and medications, providing a comprehensive view of the patient's health status. Important metrics such as vital signs, including pulse, blood pressure, and respiratory rates, are recorded to assess the patient's condition. Additionally, the form details the procedures performed, their success rates, and any medications administered, creating a clear narrative of the care provided. Billing information is included as well, allowing for a smooth process in handling insurance claims. Lastly, it contains sections for signatures, ensuring that both the patient and the service provider acknowledge the care given and any refusals of treatment. This thorough approach helps to maintain high standards of care and accountability in emergency medical situations.
Disp Type |
Service Name: (Please Print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North Dakota EMS Patient Care Report |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Service #: |
|
Unit #: |
Incident #: |
|
|
|
PCR #: |
|
|
|
Date of Onset: |
|
|
Time: |
|
|
Date Incident Reported: |
|
PCR Report Date: |
|
||||||||||||||||||
Incident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
: |
|
/ |
|
/ |
|
/ |
|
/ |
Location |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PSAP Time of Call |
|
Arrive Patient |
|
|
|
Starting Mileage |
Patient name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disposition |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Dispatched |
|
Depart Scene |
|
|
|
At Scene Mileage |
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit Role |
Enroute |
|
Arrive at Destination |
Destination Mileage |
City |
|
|
|
|
|
|
|
State |
|
|
|
|
|
Zip |
|
|
To Scene |
|||||||||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arrived at Scene |
|
Available |
|
|
|
Ending Mileage |
Phone |
|
|
|
|
|
|
|
Date of Birth |
|
|
|
|
|
Age |
|
|
|
||||||||||||||
Factor 1 |
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scene Address |
|
|
|
|
|
|
|
|
Scene GPS Longitude: |
|
|
|
|
Social Security Number |
|
|
|
|
|
Sex |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Scene GPS Latitude: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Factor 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 1 |
Scene City |
|
|
State |
|
Scene Zip |
|
Scene County |
|
|
Scene Township/FIPS |
Receiving Agency |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Complaint |
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 2 |
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
Pulse |
|
BP |
|
Resps |
GCS |
|
SaO2 |
|
EKG Interpretation |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signs and Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Factor 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
Medication |
|
|
|
Route |
|
Initial |
|
|
|
Effect |
|
|
|
||||
Dest Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 3 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dest Det |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suspected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prior Aid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Care Turned Over To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Position |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROCEDURES |
S = Successful |
U = Unsuccessful |
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
1st CPR |
|||||
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
S/U |
|
|
|
|
|
|
ATTEMPTS |
|
CREW # |
|
S/U |
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
|
S/U |
||||||
|
|
Abdominal Thrusts |
|
|
|
|
|
|
|
Delivery (OB) |
|
|
|
|
|
|
|
|
|
Needle Thorac. |
|
|
|
|
|
|
|
||||||||||||
|
|
Auto Defib. |
|
|
|
|
|
|
|
Demand Valve |
|
|
|
|
|
|
|
|
|
NG Tube |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Back Blows |
|
|
|
|
|
|
|
EKG |
|
|
|
|
|
|
|
|
|
Oropharyngeal Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Bag Valve Mask |
|
|
|
|
|
|
|
Extrication |
|
|
|
|
|
|
|
|
|
Oxygen Administered |
|
|
|
|
|
|
1st Defib |
||||||||||||
|
|
Bandage |
|
|
|
|
|
|
|
Full Spinal Immobilization |
|
|
|
|
|
|
|
|
|
Pacing |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Bleeding Controlled |
|
|
|
|
|
|
|
Intubation - |
|
|
|
|
|
|
|
|
|
Pocket Mask |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Draw |
|
|
|
|
|
|
|
Intubation Nasotrachial |
|
|
|
|
|
|
|
|
|
Splint - Extremity |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Gluc. Level Check |
|
|
|
|
|
|
|
Intubation Oro Tracheal |
|
|
|
|
|
|
|
|
|
Splint - Traction |
|
|
|
|
|
|
Shocks |
||||||||||||
|
|
Blood Product Admin. |
|
|
|
|
|
|
|
Irrigation |
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
||||||||||||
|
|
Burn Care |
|
|
|
|
|
|
|
IV Centra Vein |
|
|
|
|
|
|
|
|
|
Surgical Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Cardiovert |
|
|
|
|
|
|
|
IV Intraosseous |
|
|
|
|
|
|
|
|
|
Tourniquet |
|
|
|
|
|
|
|
||||||||||||
|
|
Cervical Collar |
|
|
|
|
|
|
|
IV Peripheral |
|
|
|
|
|
|
|
|
|
Urinary Cath. |
|
|
|
|
|
|
Race |
||||||||||||
|
|
Cold Pack |
|
|
|
|
|
|
|
MASTApplied |
|
|
|
|
|
|
|
|
|
Ventilator |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
CPR |
|
|
|
|
|
|
|
MASTInflated |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Defib - Manual |
|
|
|
|
|
|
|
Nasopharyngeal Airway |
|
|
|
|
|
|
|
|
|
Not Applicable * |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page _________of _________
Signature of Provider
Patient Name (PLEASE PRINT)
North Dakota EMS Patient Care Report
|
|
|
BILLING INFORMATION |
|
|
|
|
|
|
MILEAGE |
|
INSURANCE TYPE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance - Primary |
Number: |
Insurance - Secondary |
Number: |
|
Beg: |
|
|
|
❏ No Insurance |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Private Pay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Responsible Party: |
|
|
|
|
|
|
|
End: |
|
|
|
❏ Private Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Last Name) |
|
(First Name) |
|
|
|
(MI) |
|
Total: |
|
|
|
❏ Medicaid |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare/Medicaid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Address) |
|
|
|
|
|
|
|
|
|
|
|
❏ VA Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(City) |
(State) |
(Zip) |
|
|
(Phone) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Not Applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIPT OF SERVICE |
|
|
|
|
|
|
REFUSAL OF SERVICE |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
I acknowledge receipt of the EMS services listed in this document and accept |
This is to certify that I am refusing treatment / transport. I have been informed |
|||||||||||||
|
full responsibility for all charges. I authorize payment of medical benefits from |
of the risk(s) involved, and hereby release the ambulance service, its atten- |
|||||||||||||
|
my insurance company to provide of such services and authorize the provider |
dants, and its affiliates, from all responsibility which may result from this action. |
|||||||||||||
|
to release medical and other necessary information to my insurance company |
|
|
|
|
|
|
|
|
|
|||||
|
for that purpose. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Patient Signature |
|
|
Date/Time |
Patient Signature |
|
|
|
Date/Time |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREW |
|
CREW MEMBER NAMES |
|
|
|
|
STAFF ID |
|
DRIVER |
LEVEL |
||||
1 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EKG STRIPS
| Fact Name | Description |
|---|---|
| Form Purpose | The North Dakota EMS Patient Care Report form is used to document patient care provided during emergency medical services. |
| Governing Law | This form is governed by North Dakota Century Code Chapter 23-27, which outlines the requirements for emergency medical services documentation. |
| Patient Information | Essential patient details, including name, date of birth, age, and social security number, must be accurately recorded on the form. |
| Incident Details | Information such as incident number, location, and time of call is crucial for effective reporting and follow-up. |
| Procedures Documentation | The form includes sections for documenting medical procedures performed, including their success or failure rates. |
| Billing Information | Details about insurance coverage and responsible parties are necessary for billing purposes and must be completed accurately. |
North Dakota Form 58 Instructions - Accuracy in completing Form 58 is vital for partnerships to fulfill their tax reporting responsibilities effectively in North Dakota.
Understanding the importance of the Florida Do Not Resuscitate Order form is essential for individuals who want to make informed decisions about their healthcare, especially when it comes to ensuring their wishes are followed in emergencies. For further information and to access the necessary documentation, you can refer to All Florida Forms, which provides the appropriate resources for this critical legal process.
Nd Income Tax - Filing Form 307 is a critical step for employers to fulfill their tax reporting obligations to the North Dakota state tax authorities.
Mental Health Involuntary Commitment - The form's straightforward approach aids in demystifying the process of information submission to the government.